For many former Navy Special Warfare Combat Crewmen, the experience of delivering Navy SEALs to their destination was one of both pure exhilaration and sheer terror.
The specialized fast boats they operated could reach nearly 60 mph on the ocean. Crews could sustain these high speeds for eight to 16 hours, often under the cover of darkness, slamming into waves every few seconds.
“There were times we went out and it was so violent, each time the boat slammed at full speed, I wondered if we would fully submerge and end up killing someone,” said Anthony Smith, a former Navy boat driver.
In more than a few of those times, Smith swore he’d never go out again.
“But once you get back, you’re with all your brothers, you’d laugh about it, go drink a beer and get ready to do it again,” he said.
The specialized fast boats they operated could reach nearly 60 mph on the ocean. Crews could sustain these high speeds for eight to 16 hours, often under the cover of darkness, slamming into waves every few seconds.
“There were times we went out and it was so violent, each time the boat slammed at full speed, I wondered if we would fully submerge and end up killing someone,” said Anthony Smith, a former Navy boat driver.
In more than a few of those times, Smith swore he’d never go out again.
“But once you get back, you’re with all your brothers, you’d laugh about it, go drink a beer and get ready to do it again,” he said.
Smith said the pure adrenaline rush and the secrecy of taking down bad guys in the middle of the night were too much of a draw for him and many others.
However, the job has taken a permanent toll on operators. To better understand the extent of the injuries, Smith has independently surveyed hundreds of other veterans in the fast boat community — those who’ve operated military boats that can exceed 34 mph — and the results are overwhelming: Nearly all of the respondents claim symptoms consistent with brain injury, including anxiety, depression, sleep apnea, insomnia, testosterone problems, anger and irritability.
“There was an average of 30 comorbidities for these guys that are interconnected with traumatic brain injury,” he said, adding that he has many of the same symptoms. “Brains are destroyed. Bodies are destroyed. They can’t walk. Some of their wives are their caretakers. This is the entire [veteran fast boat operator] community.”
Smith estimates he’s logged about 12,000 hours in fast boats over his 24-year career, and he has the wear-and-tear injuries to prove it; his medical records are thick with instances of spinal injuries, joint surgeries, hearing loss and more. He has a permanent and total disability rating from the Department of Veterans Affairs. But one thing is notably missing in that rating: brain injury.
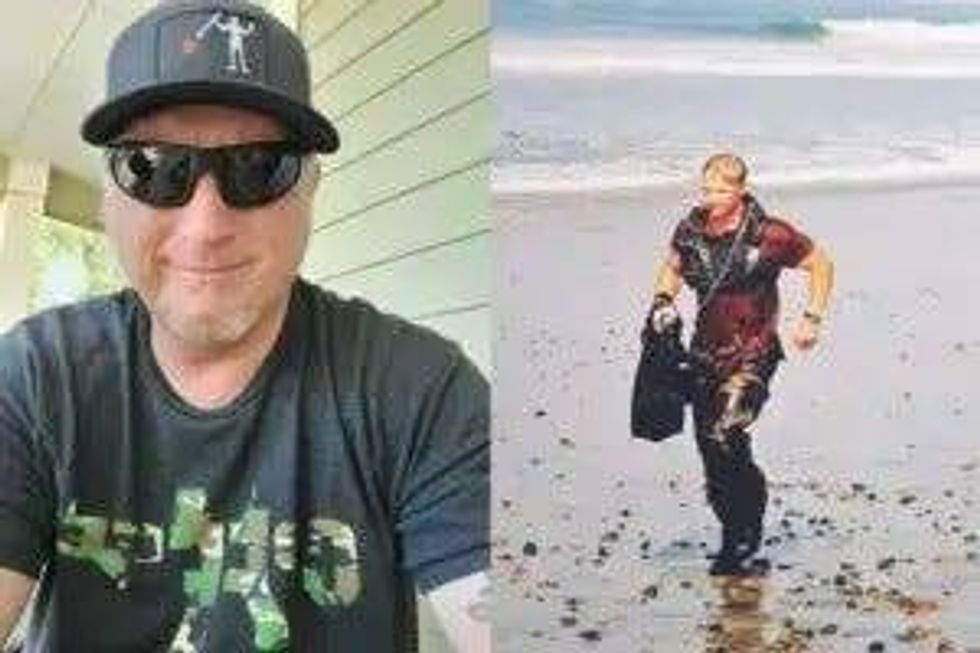 Anthony Smith is a former Navy fast boat operator who’s speaking out about the potential brain injuries caused by repeated wave slamming. He is calling on the Defense Department and the VA to conduct more research into prevention, diagnosis and treatment for them.Photos submitted to DAV by Anthony Smith
Anthony Smith is a former Navy fast boat operator who’s speaking out about the potential brain injuries caused by repeated wave slamming. He is calling on the Defense Department and the VA to conduct more research into prevention, diagnosis and treatment for them.Photos submitted to DAV by Anthony Smith
When it comes to Smith’s brain, military and VA doctors have concluded there’s nothing wrong, and if there is, they say it’s not correlated to the millions of wave impacts he’s experienced that could, at times, exceed 60 times the force if gravut to the head. exceed 60 times the force of gravity to the head. That’s the equivalent of being tackled full force by an NFL football player, a profession where brain injury is a common occupational hazard.
In the world of professional football and other high-contact sports, there have been numerous reports of athletes developing chronic traumatic encephalopathy (CTE), a brain injury caused by repeated blows to the head. It’s only diagnosable by examining a person’s brain after death but comes with a range of symptoms, including memory loss, depression, substance abuse and suicidality.
Fast boat veterans, especially those who’ve served for multiple deployments like Smith, are displaying similar symptoms. Recent reporting by the New York Times highlights fast boat veterans who died by suicide and at least one who was posthumously diagnosed with CTE.
A June 2025 study published in the American Medical Association’s open-access medical journal, JAMA Network Open, concluded that the occupational exposures experienced by Navy fast boat operators, including wave slamming, “may be sufficient to promote or otherwise contribute to the development of CTE.”
Smith puts it more bluntly: “Inside our brains is a death sentence.”
Smith said for a fast boat community numbered in the thousands, including other branches of service like the Coast Guard, not having a way to get a brain injury diagnosis means that many of the symptoms they present are often written off by military leadership as behavioral issues or something attributed to the community’s lifestyle.
They’re not the only cohort of veterans raising the warning flag about their injuries and being ignored.
Ryan Larkin was a decorated Navy SEAL who died by suicide a year after he was discharged from service. Before then, he started showing signs that something was wrong—depression, alcohol abuse and mood swings.
His father, Frank Larkin, a Navy SEAL veteran himself and retired Secret Service agent, said his son was treated for all of those symptoms with an endless flow of drugs.
“To me, it was almost like a chemical sedation just to keep him kind of in a state of suspension,” he said.
The treatments didn’t work, and Ryan kept insisting the issue was deeper.
“He said, ‘Nobody’s listening to me. Something’s wrong with my head,’” Frank recalled, adding that it got to a point where Ryan said, “I’m gonna prove that something’s wrong.”
Ryan knew he wasn’t the only one suffering without being heard, and he made sure before his death that his brain was preserved so it could be examined.
 Ryan Larkin is a Navy SEAL veteran who died by suicide a year after he left the Navy. A postmortem study of his brain revealed microscopic scarring that may be linked to repeated blast trauma and presents symptoms, including depression, mood swings and suicidalityPhotos submitted to DAV by Frank Larkin
Ryan Larkin is a Navy SEAL veteran who died by suicide a year after he left the Navy. A postmortem study of his brain revealed microscopic scarring that may be linked to repeated blast trauma and presents symptoms, including depression, mood swings and suicidalityPhotos submitted to DAV by Frank Larkin
“I don’t like what he did. I didn’t support what he did. But I’ve grown to understand,” Frank said. “He was concerned about his boys. His guys were hurt.”
Ryan’s brain was sent to Dr. Daniel Perl, a renowned brain injury expert at the Uniformed Services University’s School of Medicine in Bethesda, Maryland. Perl is a contributor to the June 2025 CTE study.
What he found in Ryan’s brain wasn’t CTE but interface astroglial scarring (IAS), a microscopic brain injury that may be linked to repeated blast trauma. It has similar symptoms to CTE and is also currently only diagnosable after death. Ryan’s job as a SEAL and special operations trainer frequently exposed him to blast forces, like those from breacher charges and high-caliber weapons.
Like Smith, Ryan’s brain injury was never diagnosed even though he had symptoms of one.
Not every fast boat operator has or will develop CTE. Not every special operator will develop IAS. But Dr. Brian Edlow, the co-director of neuroscience at Massachusetts General Hospital and a researcher studying similar brain injuries in special operations forces, said there is mounting evidence that repeated exposure to explosive blasts, blunt head impacts and acceleration g-forces (like wave slamming) is associated with a broad spectrum of cognitive, psychological and physical symptoms.
However, Edlow said there’s currently no medical diagnostic code to describe any injury associated with repeated exposure, unlike a TBI, which is the result of a single event. That’s a roadblock to getting these injuries recognized and treated.
Another roadblock is that these brain injuries are microscopic, making them undetectable with current brain scan technology.
“If a veteran seeks care for symptoms and they’re told that their brain scans are normal, that doesn’t definitively mean their brain is normal,” Edlow said. “It’s possible there’s a brain injury, but our diagnostic tests are simply not good enough to see it.”
Frank Larkin and Smith are vocal advocates for recognizing these injuries so that other veterans can get the benefits and care they need.
“We’re dealing with a whole population of veterans right now—we don’t even know the real number; 500,000 has been thrown out—of folks that may have some undiagnosed level of traumatic brain injury that may explain some of the invisible wounds that they struggle with every day,” Larkin said. “We haven’t been listening to them, and as a result, all we’re doing is just creating this wake of debris behind us that’s going to last decades.”
Larkin said the Department of Defense and the VA’s failure to listen to veterans and the lack of more aggressive research into the issue constitute institutional betrayal by a system men and women stood on the line to serve.
“And all along, they were told by the system, ‘Hey, we’ll take care of you; we’re not going to leave you behind.’ But unfortunately, that’s what’s happened,” he said.
“We know that military service is inherently a hazardous job,” said Jon Retzer, DAV’s deputy national legislative director. “When veterans speak out about their symptoms, we owe it to them to listen and not diminish their claims. We need to research and understand these types of brain injuries, find ways to prevent them and treat those in need to mitigate any long-term effects.”
Supported by the emerging evidence, the conversation around microscopic brain injuries is starting to shift, and more people, including lawmakers, are beginning to listen. As research continues, Edlow said that progress in the medical care will be built on a foundation of detection.
“We have to be able to see these brain injuries in people while they’re still alive,” he said. “I genuinely believe we’ll get there. There’s a lot of reason to be optimistic that a reliable diagnostic test is on the horizon.”
A reliable test and deeper understanding would allow for better preventative measures by the DOD, better treatment options, and validation for veterans who’ve been saying their brain is injured but can’t prove it.
“I have a high degree of confidence that if we’re able to get the diagnostics right on—being able to triage whether this is an injury or strictly a mental health kind of issue or combination of both — we’re going to give a sense of qualification to our veterans,” Larkin said.
Both Larkin and Smith say they are fighting for three main goals: Prevent these injuries in the future; find better treatment for those suffering now; and establish these brain injuries as presumptive, service-connected injuries for certain military occupations.
“We can’t leave these folks behind,” Larkin said. “We have this obligation. We can’t break our promise.”
If you or someone you know is having thoughts of suicide, contact the Veterans Crisis Line to receive free, confidential support and crisis intervention available 24 hours a day, 7 days a week, 365 days a year. Dial 988 then Press 1, text 838255 or online here.